If you attack, attack the data, not the person. It’s the data that doesn’t lie…
Fauci, under oath before Congress last week could not recall ONE PEER REVIEWED STUDY that supported the efficacy of masking.
If you attack, attack the data, not the person. It’s the data that doesn’t lie…
Fauci, under oath before Congress last week could not recall ONE PEER REVIEWED STUDY that supported the efficacy of masking.
I admit I did not fully read the article but I only saw reference to studies comparing two types of masks. Would you please point out the data in the article on these types of masks vs wearing no mask?
If the result of the study is I can relax from N95 to medical grade surgical mask, then I’m all for it. My N95s are tough to wear, I have a tight fit. All docs, patients, and visitors are required to wear surgical masks at MD Anderson Cancer Center, they give you a new one at the door, no mask no entry, and they are ok to wear all day. Covid is not burning through MDA and the patients are mostly immunocompromised, so something is working.
I found hundreds, in the interests of brevity and bandwith, I’ve just included one of them, see below; ![]() :
:
Tools
It is uncertain if medical masks offer similar protection against COVID-19 compared with N95 respirators.
To determine whether medical masks are noninferior to N95 respirators to prevent COVID-19 in health care workers providing routine care.
Multicenter, randomized, noninferiority trial. (ClinicalTrials.gov: NCT04296643).
29 health care facilities in Canada, Israel, Pakistan, and Egypt from 4 May 2020 to 29 March 2022.
1009 health care workers who provided direct care to patients with suspected or confirmed COVID-19.
Use of medical masks versus fit-tested N95 respirators for 10 weeks, plus universal masking, which was the policy implemented at each site.
The primary outcome was confirmed COVID-19 on reverse transcriptase polymerase chain reaction (RT-PCR) test.
In the intention-to-treat analysis, RT-PCR–confirmed COVID-19 occurred in 52 of 497 (10.46%) participants in the medical mask group versus 47 of 507 (9.27%) in the N95 respirator group (hazard ratio [HR], 1.14 [95% CI, 0.77 to 1.69]). An unplanned subgroup analysis by country found that in the medical mask group versus the N95 respirator group RT-PCR–confirmed COVID-19 occurred in 8 of 131 (6.11%) versus 3 of 135 (2.22%) in Canada (HR, 2.83 [CI, 0.75 to 10.72]), 6 of 17 (35.29%) versus 4 of 17 (23.53%) in Israel (HR, 1.54 [CI, 0.43 to 5.49]), 3 of 92 (3.26%) versus 2 of 94 (2.13%) in Pakistan (HR, 1.50 [CI, 0.25 to 8.98]), and 35 of 257 (13.62%) versus 38 of 261 (14.56%) in Egypt (HR, 0.95 [CI, 0.60 to 1.50]). There were 47 (10.8%) adverse events related to the intervention reported in the medical mask group and 59 (13.6%) in the N95 respirator group.
Potential acquisition of SARS-CoV-2 through household and community exposure, heterogeneity between countries, uncertainty in the estimates of effect, differences in self-reported adherence, differences in baseline antibodies, and between-country differences in circulating variants and vaccination.
Among health care workers who provided routine care to patients with COVID-19, the overall estimates rule out a doubling in hazard of RT-PCR–confirmed COVID-19 for medical masks when compared with HRs of RT-PCR–confirmed COVID-19 for N95 respirators. The subgroup results varied by country, and the overall estimates may not be applicable to individual countries because of treatment effect heterogeneity.
Canadian Institutes of Health Research, World Health Organization, and Juravinski Research Institute.
Health care workers use either medical masks, also called surgical masks, or N95 respirators for the routine care of patients with COVID-19 as a component of their personal protective equipment. Medical masks are recommended by the World Health Organization for routine care (1, 2), whereas N95 respirators are recommended by the Centers for Disease Control and Prevention for the routine care of patients with COVID-19 (3–5).
This pragmatic, randomized, open-label, multicenter trial initially aimed to assess whether medical masks were noninferior to N95 respirators for protection against COVID-19 among unvaccinated nurses providing routine care to patients with suspected or confirmed COVID-19 (see the study protocol and statistical analysis plan). The evolution of the pandemic led to protocol changes (Supplement). Before trial commencement, in addition to nurses, other health care workers were made eligible to increase enrollment, and follow-up was reduced from 12 to 10 weeks to minimize loss to follow-up. As circulation of SARS-CoV-2 increased, health care workers known to have a previous laboratory-confirmed clinical diagnosis of COVID-19 at the time of enrollment were excluded. As vaccine rollout began, participants with receipt of 1 or more doses of a COVID-19 vaccine with greater than 50% efficacy for the circulating strain (for example, messenger RNA [mRNA] or vector-based COVID-19 vaccine against the original SARS-CoV-2 strain) were excluded, and sites in Israel, Pakistan, and Egypt were added to increase enrollment. Participants that received a single dose of an mRNA or vector-based COVID-19 vaccine after enrollment (with an estimated >50% efficacy against the circulating strain) were followed until 2 weeks after their first dose and then censored. The variable follow-up time led to a change to a time-to-event analysis, and a hazard ratio (HR) was used for the noninferiority margin.
The trial enrolled participants in 29 health care facilities: 17 acute care hospitals in Canada, 4 acute care hospitals in Pakistan, 2 long-term care facilities in Israel (facilities where trained medical staff are always available to assist residents and where high-flow oxygen and medication via inhalation could be administered), and 6 acute care hospitals in Egypt. The study was done from 4 May 2020 to 29 March 2022.
The trial was approved by the Hamilton Integrated Research Ethics Board and the institutional review boards at all participating institutions. All participants provided written informed consent. The trial was restricted to health care settings where the policy was to use medical masks while providing routine care to patients with confirmed or suspected COVID-19. A data monitoring committee provided oversight of safety considerations in the trial.
Health care workers who provided direct care to patients with suspected or confirmed COVID-19 in specialized COVID-19 units and in emergency departments, medical units, pediatric units, and long-term care facilities were enrolled; intensive care units were not included in the study. Health care workers were required to spend 60% or more of their time doing clinical work when enrolled.
Health care workers were excluded if they did not have a valid fit test within the past 24 months or could not pass a fit test, had 1 or more high-risk comorbidities for COVID-19 (hypertension, cardiac disease, pulmonary disease, chronic kidney disease, diabetes, chronic liver disease, actively treated cancer, or immunosuppression due to illness or medications), had a previous laboratory-confirmed clinical diagnosis of COVID-19 at the time of enrollment, or had received 1 or more doses of a COVID-19 vaccine with greater than 50% efficacy for the circulating strain (for example, mRNA or vector-based COVID-19 vaccine against the original SARS-CoV-2 strain).
Trial participants were randomly assigned (1:1) to either medical masks or N95 respirators. Participants were randomly assigned centrally by a study statistician who generated the sequence using a computerized random number generator. Randomization was stratified by site in permuted blocks of 4. The randomization scheme was provided by an interactive web response system and performed centrally. Investigators were blinded to the group assignment, but it was not possible to conceal the identity of the medical mask or N95 respirator assignment to the study staff or participants.
Health care workers randomly assigned to the medical mask group were instructed to use the medical mask when providing routine care to patients with COVID-19 or suspected COVID-19, which aligned with the current policy in their setting. The ASTM International certified masks were provided to the health care workers either by their health care facility or by the study (Supplement Table 1). As part of the trial protocol, health care workers could also use the N95 respirator at any time based on a point-of-care risk assessment.
Health care workers randomly assigned to the N95 respirator group were instructed to use a fit-tested National Institute for Occupational Safety and Health–approved N95 respirator when providing routine care to patients with COVID-19 or suspected COVID-19. Participants were required to use the type of device they were allocated to, either a medical mask or an N95 respirator, for 10 weeks.
The intervention included universal masking, which was the policy implemented at each site. This refers to the use of a mask when in the health care facility for all activities, whether patient related or not, including in workrooms, meetings, and treating persons that were not suspected or known to be positive for COVID-19. Participants were asked to report the extent to which they used the mask that they were assigned to on a weekly basis—that is, “During your last work shift, to what extent did you wear the mask you were assigned,” where the possible responses were “Always,” “Sometimes,” “Never,” or “Do not recall.” In both study groups, health care workers were required to use the N95 respirator for aerosol-generating medical procedures, as this was in keeping with their institutional policies. In keeping with local policies, eye protection, gowns, and gloves were worn when caring for patients with suspected or confirmed COVID-19. Participants were asked to discard the medical mask or N95 respirator if it became soiled or damaged or if breathing through the device became difficult. If the institutional policy was for extended use and masks were not typically removed after a patient encounter, the extended use procedure was to be followed.
The primary outcome was time to reverse transcriptase polymerase chain reaction (RT-PCR)–confirmed COVID-19. This was measured from the date of randomization until the date of procurement of a specimen that was positive by RT-PCR. Follow-up continued until the end of 10 weeks, until 2 weeks (1 incubation period) after receipt of an mRNA vaccine, or until the date of a participant withdrawal from the trial. Laboratory personnel doing COVID-19 testing were blind to treatment allocation. Testing was done at the health care facility laboratory using health care–administered nasopharyngeal swabs. Sera from participants was obtained at baseline and at the end of follow-up and then tested for spike IgG antibodies and for nucleocapsid IgG antibodies using EUROIMMUN assays.
Secondary outcomes included serologic evidence of infection (done in participants who were seronegative at baseline and defined as a change from negative EUROIMMUN spike IgG and nucleocapsid IgG antibodies at baseline to positive nucleocapsid IgG antibody), acute respiratory illness (defined by fever and cough), work-related absenteeism, lower respiratory tract infection or pneumonia, intensive care admission, mechanical ventilation, or death. Laboratory-confirmed infection was defined as COVID-19 confirmed by RT-PCR in symptomatic participants or seroconversion.
Participants were assessed for signs and symptoms of COVID-19 through twice-weekly automated text messages. A nasopharyngeal swab was obtained if any one the following symptoms or signs was present: fever (≥38 °C), cough, or shortness of breath, or if 2 of the following were present: fatigue, myalgia, headache, dizziness, expectoration, sore throat, diarrhea, nausea, vomiting, abdominal pain, runny nose, altered taste or smell, conjunctivitis, or painful swallowing.
Adherence to the assigned medical mask or N95 respirator for routine care and to hand hygiene was measured using weekly self-reporting for all participants and external monitoring wherever feasible. Audits were done once at 3 hospitals in Pakistan and were repeated once at 2 of these hospitals within a 2-week period. They were done at 6 hospitals in Egypt where they were repeated twice at 2 hospitals and repeated once at 4 hospitals over a 4-week period. To conduct the audits of adherence to the intervention (medical mask or N95 respirator), the coordinating center randomly selected 20% of shifts at a health care facility, and during these shifts, trial participants were observed. Wearing an N95 respirator for aerosol-generating procedures was not considered during the observed audits. Reported exposures and potential exposures to COVID-19, including community and home exposure, hospital exposures, participation in aerosol-generating procedures, and hospital outbreaks (as defined by the health care facility) were measured. Participants were asked to keep diaries of signs and symptoms of respiratory illness and exposure to household and community members with respiratory illness. Cycle threshold values from patients with COVID-19, obtained while participants were on the same study units as the patients, were used to estimate viral load as a surrogate for exposure risk.
The study was powered based on the primary outcome of RT-PCR–confirmed COVID-19. For a noninferiority HR of 2, a sample size of 875 participants provided 90% power at a 0.025 significance level for event rates of 10% and an actual HR of 1. The original design estimated an event rate of 5% with a noninferiority margin of 5 percentage points (that is, up to a 10% event rate would be considered noninferior). On changing the outcome from 10-week occurrence of RT-PCR–confirmed COVID-19 to time to RT-PCR–confirmed COVID-19 so as to allow for censoring due to vaccination, the original margin on the absolute effect size corresponds to a relative effect size (HR) of 2 (see the Supplement for earlier trial design sample size calculations). A final sample size of 1010 accounted for participants who could not complete 10 weeks of follow-up because of administration of mRNA vaccine as well as for withdrawals. Hazard ratios and corresponding 2-sided 95% CIs were estimated using a Cox proportional hazards model stratifying by health care facility. The analysis fulfilled the Schoenfeld residual test for the assumption of proportional hazards in Cox analysis. The cumulative incidence of RT-PCR–confirmed COVID-19 was estimated using Kaplan–Meier methods.
Outcomes were analyzed on an intention-to-treat basis, defined by medical mask or N95 respirator assignment and follow-up until 10 weeks or 2 weeks after the first mRNA vaccine dose. Participants did not have to complete 10 weeks of follow-up to be included in the intention-to-treat analysis. Censoring was assumed independent of the randomized group assignment. No attempt was made to impute missing postrandomization values, and only observed values were used in the analysis. A post hoc analysis of the primary outcome with participants restricted to those seronegative at baseline was done using a Cox proportional hazards model stratifying by health care facility.
For serology and overall laboratory-confirmed infection, we conducted a logistic regression analysis adjusting for site to obtain odds ratios and 95% CIs. Although subgroup analyses based on pre-Omicron variant versus Omicron variant and by universal masking were planned a priori, these analyses are not reported because of potential confounding of Omicron by country and because of the mandatory policy of universal masking for all health care facilities in the trial.
A post hoc subgroup analysis was done to compare the effect of medical masks versus N95 respirators in participants with no reported exposure to household or community members with respiratory illness to those that reported at least 1 such exposure. We also conducted an unplanned subgroup analysis of the primary outcome by country. For the safety analyses, the number and percentage of participants with an adverse event according to study group are reported. For participant exposure to patients with COVID-19 or exposure to patients with suspected COVID-19, the number of exposures per week for up to 10 weeks were counted and categorized (0, 1 to 5, 6 to 10, or ≥11 exposures). The number of exposure categories per 1000 participant-days was then calculated by country and study group. Statistical analyses were done using R, version 4.2.0 (R Foundation for Statistical Computing).
The study was funded by the Canadian Institutes of Health Research, World Health Organization, and Juravinski Research Institute. The external funders of the study had no role in study design, data collection, data analysis, or data interpretation, or in writing this report.
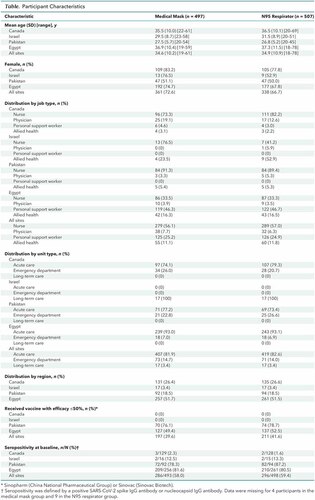
Between 4 May 2020 and 12 January 2022, a total of 1191 health care workers were assessed for eligibility, and 1009 were enrolled. There were 500 randomly assigned to medical masks and 509 to the N95 respirator (Figure 1). There were 268 participants from Canada, 34 from Israel, 187 from Pakistan, and 520 from Egypt. The baseline characteristics were well balanced overall and were similar within each country (Table). However, seropositivity at baseline varied by country, with few seropositive participants in Canada (2%) and a majority (81%) seropositive in Egypt (Table). Overall, there were 185 (37.5%) participants in the medical group versus 185 (37.2%) in the N95 respirator group who were seronegative at baseline—that is, had no SARS-CoV-2 spike IgG or nucleocapsid IgG antibodies at baseline.
Figure 1. Trial flow diagram.
ITT = intention-to-treat; mRNA = messenger RNA.
Dates of follow-up: Canada (May 2020 to May 2021), Israel (November 2020 to January 2021), Pakistan (June 2021 to December 2021), and Egypt (December 2021 to March 2022).
Table. Participant Characteristics
Follow-up began on 4 May 2020 and ended on 29 March 2022. Participants were enrolled from 4 May 2020 to 22 May 2021 in Canada, from 11 November 2020 to 27 January 2021 in Israel, from 24 June 2021 to 18 December 2021 in Pakistan, and from 19 December 2021 to 29 March 2022 in Egypt. The mean duration of follow-up was similar between the 2 study groups—9.06 weeks in the medical mask group and 9.03 weeks in the N95 respirator group. Five participants who were randomly assigned but never followed were excluded from analysis—3 in the medical mask group (1 was previously positive for COVID-19 on RT-PCR and 2 withdrew) and 2 in the N95 respirator group (1 was previously positive for COVID-19 on RT-PCR and 1 withdrew) (Figure 1). Of the resulting 1004, follow-up was complete (that is, full 10 weeks or 14 days after first vaccination) in 483 (97.1%) in the medical mask group and 489 (96.4%) in the N95 respirator group.
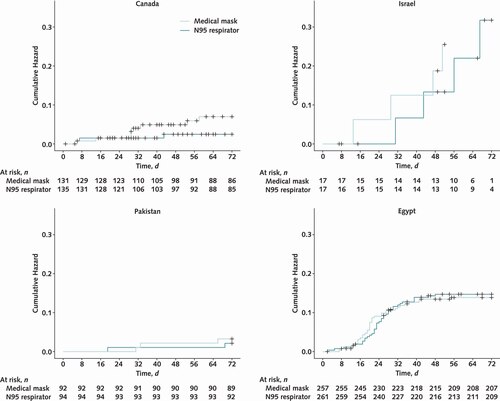
The primary outcome in the intention-to-treat analysis, RT-PCR–confirmed COVID-19, occurred in 52 of 497 (10.46%) in the medial mask group versus 47 of 507 (9.27%) in the N95 respirator group (HR, 1.14 [95% CI, 0.77 to 1.69]). The proportional hazards assumption was tested for the primary outcome and was plausible. In an unplanned subgroup analysis by country, we found that in the medical mask group versus N95 respirator group, RT-PCR–confirmed COVID-19 occurred in 8 of 131 (6.11%) versus 3 of 135 (2.22%) in Canada (HR, 2.83 [CI, 0.75 to 10.72]), 6 of 17 (35.29%) versus 4 of 17 (23.53%) in Israel (HR, 1.54 [CI, 0.43 to 5.49]), 3 of 92 (3.26%) versus 2 of 94 (2.13%) in Pakistan (HR, 1.50 [CI, 0.25 to 8.98]), and 35 of 257 (13.62%) versus 38 of 261 (14.56%) in Egypt (HR, 0.95 [CI, 0.60 to 1.50]) (Figure 2). The overall cumulative incidence is shown in Figure 3 and that by country in Figure 4.

Figure 2. Forest plot of the primary intention-to-treat analysis of RT-PCR–confirmed COVID-19.
There were 86 of 8338 (1%) weekly surveys missing in the medical mask group and 65 of 8468 (0.8%) missing in the N95 respirator group. The subgroup analysis by country was added to show the heterogeneity of treatment effect. HR = hazard ratio; RT-PCR = reverse transcriptase polymerase chain reaction.
Figure 3. Cumulative incidence of primary analysis of RT-PCR–confirmed COVID-19.
RT-PCR = reverse transcriptase polymerase chain reaction.
Figure 4. Cumulative incidence of primary analysis of RT-PCR–confirmed COVID-19 by country.
RT-PCR = reverse transcriptase polymerase chain reaction.
The secondary outcomes, which varied substantially by country, are shown in Supplement Table 2. The sensitivity analysis for RT-PCR–confirmed COVID-19 in participants who were seronegative at baseline showed within-country between-group HRs similar to those that include all participants (Supplement Figure).
Pre-Omicron exposure occurred in Canada, Israel, and Pakistan, whereas Omicron exposure occurred in Egypt. This is based on dates of SARS-CoV-2 circulation given that enrollment in Egypt began on 19 December 2021, whereas enrollment from other countries ended earlier in the pandemic, with follow-up in Pakistan ending on 28 December 2021. The post hoc intention-to-treat subgroup analysis of no reported household or community exposure to respiratory illness (HR, 1.06 [CI, 0.53 to 2.11]) versus 1 or more reported household or community exposure to respiratory illness (HR, 1.08 [CI, 0.66 to 1.78]) did not show heterogeneity of treatment effect based on a test of interaction (P = 0.96) (Supplement Table 3).
There were 2 participants who had serious adverse events in the medical mask group (both hospitalizations for COVID-19, where 1 had confirmed pneumonia) and 1 participant in the N95 respirator group (hospitalization for COVID-19 pneumonia). In addition, there were 3 participants (2 in the medical mask group and 1 in the N95 respirator group) who could not be safely isolated at home and were hospitalized for isolation. There were no intensive care admissions and no deaths. There were 47 (10.8%) adverse events related to the intervention reported in the medical mask group and 59 (13.6%) in the N95 respirator group (Supplement Table 4). There was 1 participant in the medical mask group and 3 in the N95 respirator group who withdrew because of discomfort or adverse events related to the device they were assigned.
Exposure to patients with confirmed or suspected COVID-19, minutes of exposure to patients with COVID-19, aerosol-generating procedures, and community exposures were similar between study groups (Supplement Tables 5 to 9). Mean cycle threshold values of patients positive for COVID-19 were less than 30 in 84% of the 25 study units where these data were collected (Supplement Table 10). Ventilation in the study varied by location (Supplement Table 11). Outbreaks of COVD-19 were reported in 5 of 29 (17%) study units in Canada, in both long-term care facilities in Israel, and in all 6 acute care hospitals in Egypt (Supplement Table 12).
Adherence with the assigned medical mask or N95 respirator was self-reported as “always” in 91.2% in the medical mask group versus 80.7% in the N95 respirator group and as “always” or “sometimes” in 97.7% in the medical mask group versus 94.4% in the N95 respirator group (Supplement Table 13). Of 118 participants observed in the medical mask group, 116 (98.3%) were reported by monitors to be adherent to their assigned mask—14 (100%) in Pakistan and 102 (98%) in Egypt. Of 117 observed in the N95 respirator group, 113 (96.6%) were reported to be adherent—8 (80%) in Pakistan and 105 (98%) in Egypt (Supplement Table 14). Self-reported rates of adherence to hand hygiene, eye protection, use of gowns, and use of gloves were similar between study groups (Supplement Table 13).
Among health care workers who took care of patients with suspected or confirmed COVID-19, although the upper limit of the CIs of the pooled estimate for medical masks when compared with N95 respirators for preventing RT-PCR–confirmed COVID-19 was within the noninferiority margin of 2, this margin was wide, and firm conclusions about noninferiority may not be applicable given the between-country heterogeneity.
The heterogeneity in the RT-PCR positivity rate, as well as the heterogeneity in baseline seropositivity by country, may be explained by many factors. Enrollment in Canada occurred early in the pandemic in acute health care facilities. In contrast, in Israel, the study was done in long-term care facilities that had substantial outbreaks. Later in the pandemic, enrollment occurred in Pakistan and Egypt, countries with a high population density, where seropositivity in participants due to previous exposure to SARS CoV-2 and receipt of vaccine was more common. Circulation of Omicron may have been a contributing factor to the high rates of RT-PCR–confirmed COVID-19 in Egypt.
The observed results are consistent with a range of protection, from a 23% reduction in the HR with medical masks to a 69% risk increase. The relative protection of medical masks compared with N95 respirators varied by country. However, this finding does not seem to be explained by differences in baseline seropositivity given that a post hoc analysis of the effect of medical masks versus N95 respirators on RT-PCR–confirmed COVID-19 that was restricted to participants seronegative at baseline led to similar within-country point estimates compared with analyses that included the seropositive participants.
Although self-reported adherence was lower in the N95 respirator group, the randomly conducted audited adherence was similar in both groups—98.3% in the medical mask group versus 96.6% in the N95 respirator group. It should be noted that the intervention included the mask policy at each site and not only the type of mask to which participants were randomly assigned. It is possible that the type of mask influenced adherence, which would be intrinsic to the pragmatic nature of the trial. We acknowledge concerns of suboptimal filtering capacity of medical masks, but the trial was done strictly in settings where the policy was use of medical masks for routine care, and no participants who were using N95 respirators were asked to use medical masks. In Pakistan and Egypt, the trial offered superior-quality medical masks and N95 respirators to participants who would otherwise not have access. High-risk participants were excluded from the study, and the data were routinely monitored by the Data Safety Committee. Furthermore, participants who believed they were at high risk during a particular exposure were allowed to use the N95 respirator if assigned to a medical mask.
In conclusion, among health care workers who provided routine care to patients with COVID-19, the overall estimates rule out a doubling in hazard of RT-PCR–confirmed COVID-19 for medical masks when compared with HRs of RT-PCR–confirmed COVID-19 for N95 respirators. The subgroup results varied by country, and the overall estimates may not be applicable to individual countries because of treatment effect heterogeneity.
I don’t know why I bother. I’m not going to convince anyone. My last shot:
The article you presented was not a mask efficiency study it was a comparison of the surgical mask with the N95 mask. Hence not a mask efficiency study.
It has a conclusion of 10.46% with Covid after the 10 week period who had medical (surgical) masks. There was 9.27% with Covid in the N95 masks. So the conclusion is NO DIFFFERENCE, like I stated.
Problems with the study you presented, for further review:
Amen. Done. No more time wasted.
Icarus
I only glanced at the report. However, I know data can be misinterpreted.
When I see that medical professionals used two types of masks and there is little difference between them, my first thought is, what about non-medical experts? Is one type of mask asier to be mis-worn by the public than the other? For example, those masks at Costco (the black ones) are just folded material, where the better grade masks I see people wearing actually form fit to the nose and mouth causing a cone. It is more difficult to mis wear that type than the folded ones. The folded type I have seen people flip over and wear inside out.
I would rather get a vaccine than not (in the 50’s my next door neighbor had Polio).
I say “Money isn’t everything, but it is way ahead of what is in second place!”. The masks may not be a perfect solution, but I would rather wear one than not.
Thank you!
I never let the perfect be the enemy of the good
The Cook Islands has had a similar experience to yours, albeit on a much smaller scale. Here’s the report from the World Health Organization. It’s backed up by personal anecdotal information from Cook Islander friends with whom we regularly communicate.
The report states: “In Cook Islands, from 3 January 2020 to 5:46pm CET, 5 December 2022, there have been 6,389 confirmed cases of COVID-19 with 1 deaths, reported to WHO. As of 10 May 2022, a total of 39,612 vaccine doses have been administered.”
That data presents a pretty compelling evidence supporting the effectiveness of the COVID vaccines because just about everyone, (well over 95% of the population) got vaccinated.
Wow, 1 death in 17,500.
Texas… 92,300 deaths, population 29,145,505. That’s 1 death in 316.
Hmmm… sucks to be us. As usual, we failed the intelligence test.
Given that the wearers were not vaccinated, the data would indicate around 90% effectiveness for people who were likely exposed to an above-average level of infected people.
Its a very nice advantage to be able to completely shutoff people traveling to your state…the benefit of being an island (group of islands). The rest of the US doesn’t have that luxury…and the open national borders don’t help either.
I’ve spent a lot of time in the Cook Islands, roughly 15 visits of between 3 to 8 weeks in duration each and I lived in Texas for seven years.
Knowing the residents pretty well in each of the two locations, the difference in COVID deaths is pretty easy to understand.
Is it a nice tourist destination?


{kind=link}
{kind=link}
{kind=link}
{kind=link}